
Treatment
Myasthenia gravis is one of the most treatable neuromuscular disorders. The choice of treatment depends on several factors including
- age, overall health,
- severity of disease,
- rate of disease progression.
Physicians now estimate that if myasthenia gravis is treated the mortaility rate is zero. Most sufferers of the disease are able to lead active lifes and manage their symptoms. In myasthenia gravis there are few AChR sites on the muscle and therefore the ACh is broken down before it can fully stimulate the muscle resulting in muscle weakness.
Acetylcholinesterase inhibitors
Acetylcholinesterase inhibitors are typically the first line treatment of Myasthenia Gravis. These medications increase the level of acetylcholine available at the neuromuscular junction by impairing the breakdown of acetylcholine at the synaptic cleft.
Prostigmin
Prostigmin (neostigmine bromide), an anticholinesterase agent, is available for oral administration in 15 mg tablets.
Pyridostigmine
Pyridostigmine inhibits acetylcholinesterase in the synaptic cleft, thus slowing down the hydrolysis of acetylcholine. The effects of pyridostigmine may be noticed 15 to 30 minutes after taking a dose. The typical starting dose is 30 mg three times a day the beneficial effects last for 3 to 4 hours. For some patients the effects of the symptoms disappear with pyridostigmine alone, however most require additional treatments, which vary for each patient.
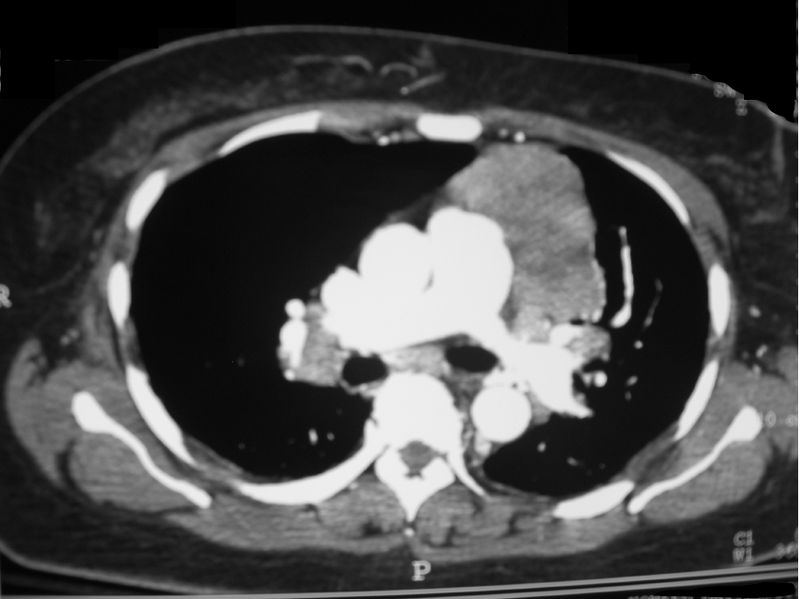
Thymectomy
Surgical removal of the thymus is usually recommended in patients who have a thymoma. A Thymectomy may also be beneficial in patients who develop the disease under 45 years of age, this is because in these patients the thymus is one of the places where the antibodies against the AChR are made. Following a thymectomy improvement of symptoms may become apparent after the first year usually however it can take upto three years. If the patient recovers or improves significantly following the operation they may not require additional therapy however in many cases patients need further treatment.
Immunosuppresion

Steroids
Patients who do not respond to thymectomy, or do not undergo a thymectomy, are often treated with steroids. Patients usually are started on a low dose of steroids, which is gradually increased over the following two weeks to reach the full dose. Once the symptoms are controlled, the dose of steroids is gradually reduced this is to find the minimum dose at which the symptoms remain under control. Patients are then maintained on that dose - as the most sutiable for that individual. There are several side effects associated with steroids e.g. Osteoporosis however additional medication can be given to help prevent these side effects.
- E.g. Prednisolone
Plasmapheresis and immunoglobulin therapy
This method of treatment if only used if the muscle weakness caused by myasthenia gravis becomes so severe that it causes problems in breathing or swallowing. Both methods of treatment are not used for long term treatment as there results only last for a period of a few weeks. However they both significantly improve the patients symptoms during that period of time.
Plasmapheresis
The blood of the individual is routed through a machine which removes the plasma- it is this plasma that contains the harmful antibodies, the individuals antibodies, the plasma is replaced with antibody free plasma reducing the autoimmune response.
Immunoglobulin therapy
The individual who is suffering from myasthenia gravis is injected with normal functioning antibodies- ones which wont attack the patients AChR.
This video is courtesy of Root atlas under the creative commons license
The image courtesy of Tom Varco under the creative commons license
A-P Xray of Thyroma courtesy of Wikicommon under creative commons license